The Sphenoid Bone
The sphenoid bone is one of the eight bones that make up the cranium – the superior aspect of the skull that encloses and protects the brain.
Its name is derived from the Greek ‘sphenoeides’, to mean wedge-shaped.
In this article, we shall look at the anatomy of the sphenoid bone – its location, structure, and clinical significance.
By TeachMeSeries Ltd (2019)
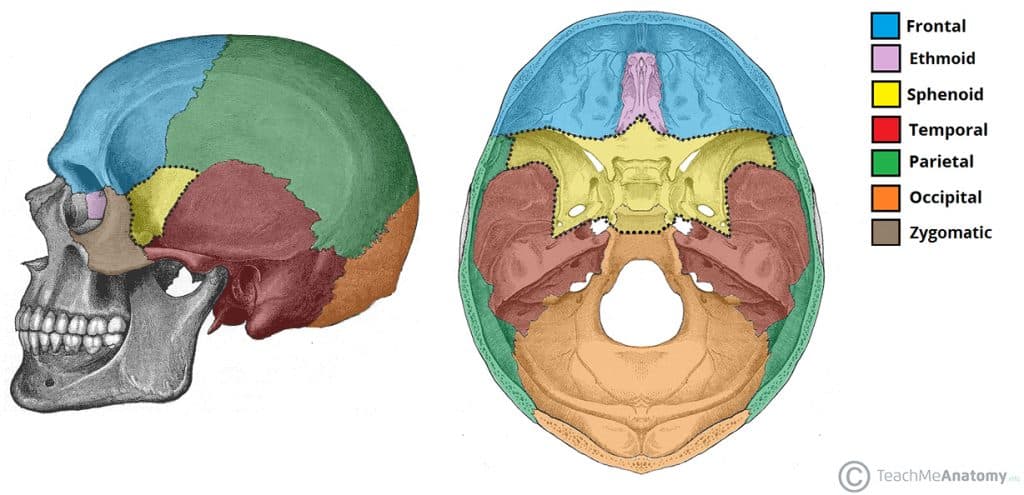
Fig 1 – The position of the sphenoid bone (yellow) within the facial skeleton.
Anatomical Structure
The sphenoid bone is said to be ‘butterfly-shaped‘. It consists of a body, paired greater wings and lesser wings, and two pterygoid processes.
Body
The body lies at the centre of the sphenoid bone, and is almost completely cubical in shape.
It contains the sphenoidal sinuses, which are separated by a septum – meaning that the sphenoid body is essentially hollow. The body articulates with the ethmoid bone anteriorly, and it is here that the sinuses open up into the nasal cavity.
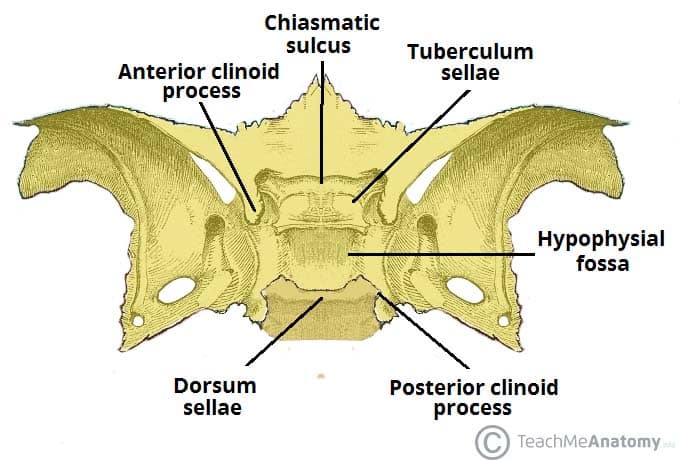
The superior surface of the sphenoid body contains some important bony landmarks:
- Sella turcica – a saddle-shaped depression. It has three parts:
- Tuberculum sellae – forms the anterior wall of the sella turcica, and the posterior aspect of the chiasmatic groove.
- Hypophyseal fossa – the deepest part of the sella turcica, where the pituitary gland is located.
- Dorsum sellae – forms the posterior wall of the sella turcica.
- Chiasmatic groove – a sulcus formed by the optic chiasm (where the optic nerves partially cross).
The sella turcica is surrounded by the anterior and posterior clinoid processes. The anterior clinoid processes arise from the sphenoidal lesser wings, while the posterior clinoid processes are the superolateral projections of the dorsum sellae. They serve as attachment points for the tentorium cerebelli, a membranous sheet that divides the brain.
By TeachMeSeries Ltd (2019)
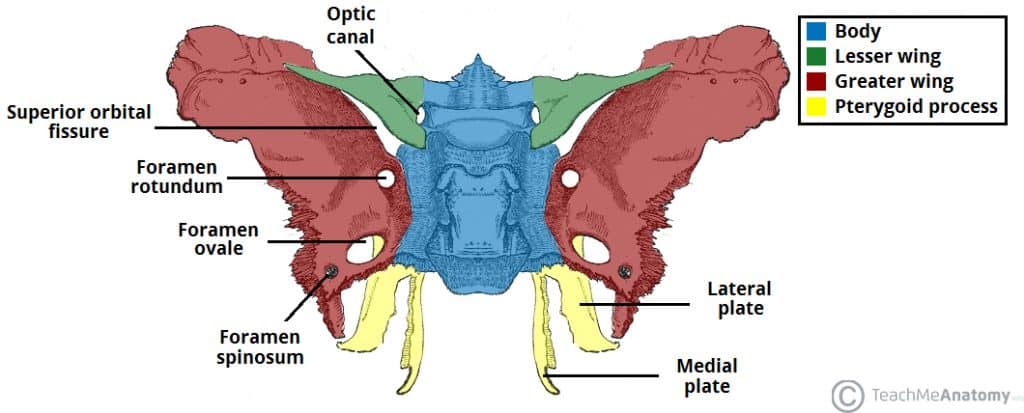
Fig 2 – Foramina and bony landmarks of the sphenoid wings and pterygoid process.
Greater Wing
The greater wing extends from the sphenoid body in a lateral, superior and posterior direction. It contributes to three parts of the facial skeleton:
- Floor of the middle cranial fossa
- Lateral wall of the skull
- Posterolateral wall of the orbit
There are three foramina present in the greater wing – the foramen rotundum, foramen ovale and foramen spinosum. They conduct the maxillary nerve, mandibular nerve and middle meningeal vessels respectively.
Lesser Wing
The lesser wing arises from the anterior aspect of the sphenoid body in a superolateral direction. It separates the anterior cranial fossa from the middle cranial fossa.
It also forms the lateral border of the optic canal – through which the optic nerve and ophthalmic artery travel to reach the eye. The medial border of the optic canal is formed by the body of the sphenoid.
There is a ‘slit-like’ gap between the lesser and greater wings of the sphenoid – the superior orbital fissure. Numerous structures pass through here to reach the bony orbit.
Pterygoid Process
The pterygoid process descends inferiorly from the point of junction between the sphenoid body and the greater wing. It consists of two parts:
- Medial pterygoid plate – supports the posterior opening of the nasal cavity.
- Lateral pterygoid plate – site of origin of the medial and lateral pterygoid muscles
Muscular Attachments
The lateral and medial pterygoid muscles which form some of the muscles of mastication originate from the lateral pterygoid plate of the sphenoid bone.
Articulations
The sphenoid is an unpaired bone. It sits anteriorly in the cranium, and contributes to the middle cranial fossa, the lateral wall of the skull, and the floor and sides of both orbits.
It has articulations with twelve other bones:
- Unpaired bones – Occipital, vomer, ethmoid and frontal bones.
- Paired bones – Temporal, parietal, zygomatic and palatine bones.
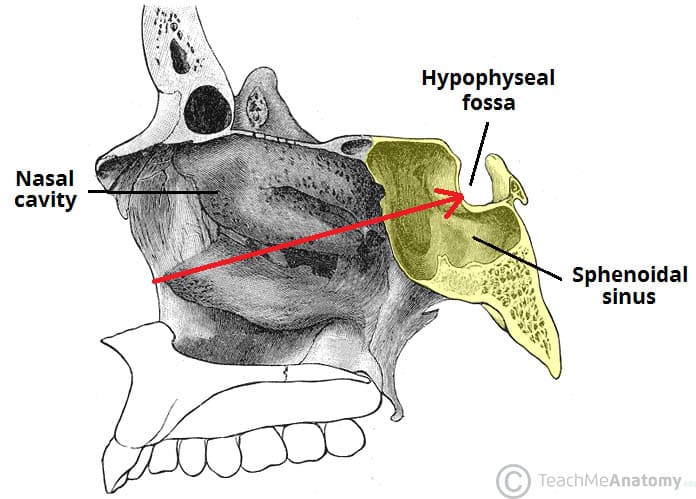
Clinical Significance - Transsphenoidal Surgery
The sphenoid bone shares a close anatomical relationship with the pituitary gland. Indeed, the pituitary can be accessed surgically by passing instruments through the sphenoid bone and sinus.
This type of surgery is known as endoscopic trans-sphenoidal surgery (ETSS), and is the usual treatment of choice for pituitary adenomas. It allows for the surgical management of pituitary pathology without the need for a more extensive craniotomy.
Comments
Post a Comment